HackerNoon Editor’s note: As the author of this article themself admits, they are NOT a doctor or a medical professional. What you are about to read is based on their OWN personal research, and MUST be considered anecdotal, even when the author cites another medical professional’s material to lend credence to their claim. As such, you should ALWAYS seek medical advice from a certified professional. The HackerNoon editorial team has only verified the story for grammatical accuracy and does not condone/condemn any of the claims contained herein. #DYOR
Baby-making is more complicated than it might seem, and any couple struggling to conceive and achieve a successful pregnancy is faced with a confusing maze of fertility optimization measures.
This is where whole genome personal genotyping can be very helpful. Your genes obviously have everything to do with fertility, and your genes are unique. Personal genotyping can illuminate what you might be doing wrong in the fertility optimization department. It empowers you and your partner to practice precision Biohacking by identifying the medicine, supplements, therapies, and lifestyle changes you need to bring a beautiful baby into the world.
I’m not a doctor, just a Biohacker who has been obsessively researching this topic, for the last couple of years, to build my own family. This is NOT a replacement for a doctor’s guidance on your parenting journey.
This article will elucidate 17 problematic fertility genes you may have, how to find them, which conditions they are associated with, and give you a jumping-off point for addressing them…
My lovely wife and I are veteran Biohackers, so we’ve already implemented most of the “low-hanging fruit” fertility optimization things, but we remain aspirational parents in our late 30s, so we got our personal genotyping done to guide our journey in producing the next generation of little Roselands.


We chose Sequencing.com for whole genome sequencing and genetic analysis for the reasons detailed here…
I’m not an affiliate or official brand ambassador of Sequencing.com. My only affiliation with them is that I read and reviewed Dr. Brandon Colby’s book, Outsmart Your Genes (which he wrote before founding Sequencing.com), on personal genotyping, which he appreciated and reciprocated by extending us two free kits. I do think they are currently the best personal genotyping service, and would have paid for it were Dr. Colby not so generous, as I appreciate their iron-clad Privacy Forever policy.
An important disclaimer:
- Do you experience symptoms of this condition?
- Does this condition affect others in your family?
- Do your blood testing panels hint at this condition?
- Has your doctor diagnosed you with a condition?
- Have you optimized your diet and lifestyle to account for this condition?
If the only place this condition shows up in your life is your genome report, it may be a gene that’s not expressing itself.
How to search your genome
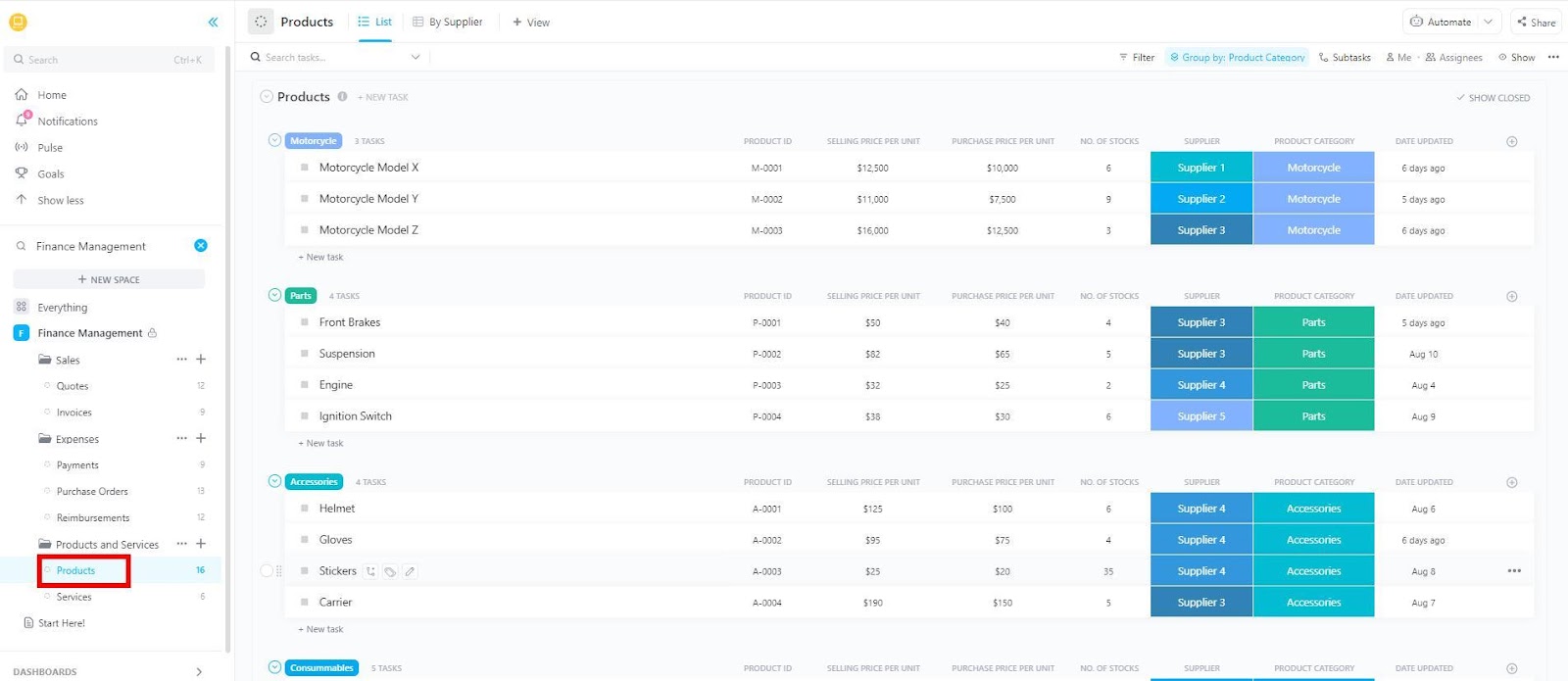
Diving into your genes may seem intimidating, but the Sequencing.com dashboard makes it pretty easy. Start by navigating to your genome explorer and cross-reference conditions by fertility. The genomics provider you select should have a similar function. As you can see here, Sequencing.com crucially differentiates the scientific confidence of the evidence linking your genes and the conditions that may impact your fertility. You don’t want to majorly freak out about a potential condition that is loosely linked to genes merely by preliminary scientific studies.


No single gene is “bad” – they are all there for a good reason, but you may have variants of them that you need to account for in your fertility optimization. In this article, I include individual problematic variants/mutations (SNPs), but there are thousands and thousands of them impacting fertility, and (shocking admission) I may be wrong (or the current science on them might be wrong). Your genotyping will let you know just which ones you have and should include links to the up-to-date scientific evidence that correlates your variations to potential fertility challenges.
After cross-referencing by fertility, you’ll want to cross-reference your genome by single gene disorders and polygenetic complexes (bolded below) that impact fertility, which we’ll turn our attention to now…
Single gene disorders


According to Sharyn Lincoln, a certified genetic counselor, Fragile X is one of the most common single-gene causes of primary ovarian insufficiency, as is galactosemia (but less common). Chromosomal abnormalities and other genes that may contribute to ovarian insufficiency are BMP15, NOBOX, NR5A1, and FIGLA.


What to do if your genes predispose you to ovarian insufficiency…
- The obvious solution is to have children earlier rather than later in life, especially if your genes predispose you to ovarian insufficiency – it becomes a greater challenge to fertility as the woman approaches 40 years old. If you don’t have a virtuous person around to make a baby with, “freeze your eggs.”
- Several Mitochondrial nutrients – CoQ10, Resveratrol, and Melatonin – may slow down ovarian aging.
- Interestingly, there’s some scientific evidence for solutions out of Chinese traditional medicine – notably Bushen Culuan Decoction in combination with clomifene citrate.
- Look into Stem Cell Based Therapies to Promote Follicle Development, discussed here.
On procrastination (the enemy in your sacred mission to become the great mother or father you can be)
The 13 bolded words of the bullet point above may have triggered you a bit, especially if you’re like my wife and I and you’ve procrastinated some in becoming a parent. If you have, looking in the mirror and taking some responsibility for that procrastination will serve you on the journey to joyous parenthood ahead of you. The time for procrastination is over. It’s now time to take this thing seriously; don’t be shy about spending time, resources, and money on fertility optimization. And don’t be shy about employing good fertility doctors and genetic counselors to help you make sense of your genotyping results. After reading this article, you and your partner will be especially empowered to take your destiny and legacy into your own hands. I wrote elsewhere that…
I tend to think that the universe bends to the will of the man or woman determined to impose it with absolute belief. And actually, that’s the most proven fact in science with over 150,000 gold-standard clinical trials proving the power of belief [the “placebo effect”] over the material structure of our biology (fixing broken bones and curing cancer, to mention a few things)…
in this article, we’ll explore more the surprising role that the placebo effect can have in your babymaking journey.
Polygenetic complexes


This is a fancy way of saying that there are genetic and environmental factors influencing infertility with these conditions. Determining causality for these is tricky, but if these complexes show up commonly in the woman’s family, they are likely a genetic factor.
Endometriosis – There is not a clear genetic test for Endometriosis, but there are some candidate genes – it’s associated with the PAI gene, discussed below.
Polycystic ovarian syndrome (PCOS) – There is not a single genetic cause of this one, but in its nonclassic form, PCOS can cause infertility. The genetic condition congenital adrenal hyperplasia, which you can search for in your genome report, can sometimes masquerade as PCOS, and it’s associated with CYP11B1. PCOS doesn’t damn you to a childless life, and addressing it is a broad topic beyond the scope of this article, but if your PAI gene is red-flagged, here’s a jumping-off point for Biohacking it.
Fibroids – Associated with the MED12, HMGA2, and COL4A5 genes, are very common in the general population and do not necessarily impact fertility. Fibroids sometimes result from a single-gene condition, Hereditary Leiomyomatosis, and Renal Cell Cancer (HLRCC), which is caused by the FH gene, which is also associated with a renal cancer predisposition. The lifestyle options for preventing or treating Fibroids include reducing system inflammation and avoiding estrogenic foods, and apparently, the ECGC in green tea can shrink them. In some cases, myomectomy (surgical removal of fibroids) should be considered.
Triple X Syndrome – When the woman has an extra X chromosome. This is rare but more common in tall women and may impact fertility, implicated in lower-than-average estrogen levels and elevated risk for premature ovarian failure. Triple Xers may struggle with hormonal balance, so get your hormones tested: importantly, ovarian reserve markers like AMH (Anti-Mullerian Hormone) and FSH (Follicle Stimulating Hormone). If there’s significant room for improvement, consider: increasing dietary Phytoestrogens (like flaxseeds and lentils), taking the progesterone-regulating herb Vitex (Chasteberry), and supplementing DIM (Diindolylmethane) which helps balance estrogen levels.
MTHFR
Is probably the most well-known gene; it’s described as the “master switch” for many of our body’s biochemical pathways by researcher Carolyn Ledowsky of MTHFR Support Australia, a fertility center. It determines how you methylate folate, and it has a lot to do with fertility.


Genetic nutritionist and author Russell Browne names it as the #1 “infertility gene.” You can cross reference your personal genotyping report by these problematic mutations (named in Browne’s book): C677T, C24909T, A4598G, A4117C. And A1218C and S67TT are also associated with fertility challenges.
You may already know that if you’re an MTHFRer, the garden variety folic acid supplements are useless to you, along with other non-methylated vitamins like the cyanocobalamin form of B12. Well, Dave Asprey makes a strong case in The Better Baby Book that every woman should choose Folinic acid – the most bioavailable form.
Niacin– 100 mg
Riboflavin (FAD)-100 mg
Vitamin B6 (P-5-P)– 25 mg
Magnesium Bis-glycinate5-MTHFR(L-methyl-folate) or “Activated Folate” – This one can be a double-edged sword; take it with the guidance of your doctor (who should be well educated on MTHFR). And it could be problematic for those with a history of mental health issues.
ZincB-complex vitaminFolinic acid
Along with eating methylation-supporting foods: eggs, beets, wild-caught salmon, and beans. And mind your gut health; get your gut microbiome analyzed to see which probiotic strains you really need (you’ll have to send a poop sample to a service like Viome), eat probiotic foods daily, maybe use the peptide BPC-157, and take a few deep relaxing breaths before every meal (it’s a digestion hack).
If you struggle with fatigue, that’s a tell-tale sign that you’re not methylating correctly.
SLC19A1
A few variations of this gene can cause issues with folate getting into cells. If your genotyping turns up red flags for this gene, you’ll need additional Vitamin B1 to ensure that folate production is not being inhibited.
DHFR
This gene is a lesser-known member of the folate-regulating family of genes, but it has everything to do with the essential methylation mechanism. MSH T-473A is a problematic variant, according to Browne, if you got it you’ll want to avoid folic acid, grape seed extract, and ECGC (so no red wine or green tea, bummer!). Niacin supplementation is a good idea. Also, apparently, this gene is particularly vulnerable to radiation (all that terribly convenient EMF radiation from our smartphones, wifi, and laptops – you DHFR doesn’t like it!) – so take the EMF-mitigation measures described here seriously.
MTR and MTT
These are important Vitamin B-12-related genes that govern how your body uses the essential vitamin; they work together to convert cobalamin into methylcobalamin. They also interact with the folate cycle. The common lab reference ranges underestimate how much B12 you need; shoot for at least 500 – 900 pg/mL serum B-12 to properly support methylation. Is it as simple as getting a prick in the arm checking your blood serum levels to ensure you’re in good shape? Unfortunately not. The map is not always the territory with B12 deficiency, according to Browne. If your personal genotyping turns up red flags for these genes, merely taking more B-12 might not be the answer – your body might not be absorbing it. What other steps can you take to optimize your B-12 genes…
- Zinc is an important cofactor for MTR
- SAM is MTRR’s cofactor – of which Niacin is a source
Take the right form of B12 for your genes…
- Hydroxocobalamin – the most common form that’s fine for most people.
- Methylcobalamin – A more bioavailable form that shortcuts the MTRR-regulated metabolism, but not for those with COMT gene-related mental health issues
- Adenosylcobalamin – Ideal for those who have gene mutations in MUT, MMA, MMAB, MMADHC, or who have elevated (Methylmalonic acid) MMA on a blood test
TCN
Certain mutations of this gene may have deleterious effects on your uptake and utilization of Vitamin B12: Notably TCN1 G4939288A and TCN2 C766G. Try taking B12 in liposomal form or via nasal drops if it’s hard to get your B12 levels on blood tests into a healthy range.
PAI/SERPINE1
This stands for Plasminogen activator inhibitor and is the gene responsible for blood coagulation and clotting. The PAI-1 4G/5G polymorphism is associated with thrombophilia and Endometriosis. Your personal genotyping will turn up problematic variants that you may have with PAI or SERPINE1. If it’s “broken,” commonly meaning overactive, this can increase the risk of blood clots, resulting in implantation failure or miscarriages. Steps to take to mitigate the associated risk of thrombophilia and PCOS…
- Take anti-coagulants that will thin the blood: low-dose aspirin or heparin commonly. Heparin is an injectable pharmaceutical drug, you might ask your doctor about instead using low molecular weight heparin (LMWH) which is associated with fewer side effects and longer-lasting action. The good news is that there are some natural alternatives to Heparin: Nattokinase, omega-3 fish oil, garlic, and curcumin (COA-verified as heavy metal free, NOT the cheap stuff at the grocery store).
- Biohack insulin sensitivity: insulin resistance is a factor in both PCOS and thrombophilia. Addressing insulin resistance would start with lifestyle changes: weight management, fasting, and improving diet. Metformin is commonly prescribed to treat PCOS, but Metformin is a complicated cat (I’m not convinced it always does more good than harm). I would first address insulin resistance with Berberine HCL, Citrus Bergamot Extract, Inositol (particularly the Myo-inositol and D-chiro-inositol forms), or homeopathic Metformin (yes, this is a thing. And there is some evidence for its safety and efficacy). The major Biohack for insulin resistance is taking a stack of NMN and Pterostilbene or Resveratrol (check out the Epigenetic Awesomeness Protocol – I would take 500 milligrams of NMN, a capsule of Pterostilbene, and enjoy a glass of organic red wine at dinner).
- Vitamin D plays a role in regulating this gene, so get your D3 levels tested and take steps to get into a healthy range.
- Women with the 4G/5G polymorphism should be closely monitored by their physician during pregnancy to manage clotting risks and optimize outcomes.
PEMT
Is the gene that makes Choline, which is essential to pregnancy, especially during the first trimester when the baby’s brain is forming. Your genotyping will reveal if you have a problematic PEMT variant. If you do, you do; good news, this is an easy one to account for by increasing your choline intake via dietor supplementation. Phosphatidylcholine or Alpha-GPC is the most bioavailable form (and a Nootropic – it may make you a wee bit smarter).
And get a hair-mineral analysis done to see if you are deficient.
APEO
This is the gene that builds your baby’s brain, so it’s pretty important. You want your baby to be a smart cookie, right? Your genotyping may turn up the problematic APEO4, G5964A, and IVS1+69 variants, which means that you’ll need more healthy fats. If you can’t eat wild-caught salmon once or twice a week, take a high-quality Fish Oil supplement to get the EPA+DHA content you need. Krill Oil and Cod Liver Oil are the Mercedes and BMW of fish oils – I’d choose those!
Good news, Chlorella and Spirulina contain DHA. Given the choice, I’d rather get my DHA from these supplements as they also chelate toxins and can be consumed powdered as a pleasant herbal tea. That sounds better to me than trying to figure out which omega-3 fish oil supplements are legit.
FVL and F2
Blood clots are bad news in pregnancy, and these are the variants that regulate clotting in a problematic way. This is why the father also needs to be genotyped; his carrying the Factor V Leiden (FVL) or Prothrombin (F2) varients can raise miscarriage risk.
If you or your partner have these, it’s important to mitigate risk factors: obesity, sedentary lifestyle, elevated cholesterol, smoking, and poor diet. You should also test for platelets, C-reactive protein, and fibrinogen. Avoid unnecessary hormone therapy – it can worsen things. Supplement Niacin and Fish Oil to vasodilate and thin blood.
NOS
These genes regulate Nitric Oxide production and Nitric Oxide is a double-edged biological sword. The problematic G6797A and T786C variants can result in the downregulation of Nitric Oxide, which impacts the oxygen your growing baby needs. Get enough of the Nitric Oxide cofactors: Riboflavin, iron, and arginine (eat quality dark chocolate). But don’t go crazy with Nitric Oxide supplements; get your oxidant/antioxidant balance tested – you may need more antioxidants. Also, if your genes predispose you to an oxygen deficiency, get more intentional about your breathing; do 10-20 minutes of breathwork a day to teach yourself to breathe deeper (it will help your stress levels), and do mouth taping at night to habituate nose breathing.
GST/GPX
You’ve heard of Glutathione, the master antioxidant, and these are the genes that regulate it. Your personal genotyping will turn up any problematic variants, which may mean that your body is not detoxifying sufficiently. Steps to take to support Glutathione: increase B2 and selenium (enjoy a Brazil nut or two daily). And, of course, you can supplement Glutathione itself; N-acetylcysteine (NAC) is a popular source of Glutathione, but some do not respond well to taking it all the time. I take NAC during the colder months to support immunity, but S–Acetyl L–Glutathione or a liposomal supplement is a better option for getting the Glutathione you need.
Do a hair-mineral test to get an idea of how many toxic heavy metals you have in your body. If you’re pretty toxic (most of us are) and carry problematic variants of this gene, you really need to step up your detox efforts…
- Include a lot of chelating foods in your diet (which will claw out the toxins): Add some fresh Cilantro to everything it goes well with (which is practically everything!), along with powdered Chlorella and Spirulina. And eat a strawberry after enjoying some sushi.
- Supplement Quercetin, Astaxanthin, and you could try the “most beautiful molecule” C60 – it’s a powerful detox agent.
- Sweat more at the gym, on your home exercise bike, doing the horizontal tango in the bedroom, or in a sauna.
- Avoid mold. Do you have bad dreams often, and does your bathroom always smell funny? Get your home mold-tested and consider moving.
- Follow a detox protocol under the supervision of your doctor (a doctor who knows their stuff when it comes to detox – this a good place to turn to naturopath).
To go deeper on the topic of standing up to the toxicity of modernity and avoiding toxins in the first place, check out my deep-dive book review of Food Forensics.
PON
The gene is what keeps your liver doing its detox thing, dealing with all the nasty organophosphates (pesticides and insecticides, other nasty toxins that the “geniuses” in Big Agriculture stuff into almost all the food you can find at the grocery store). This toxicity accumulates in your body, resulting in infertility and potentially birth defects. If your personal genotyping red flags this gene (particularly if you have the PON1 Q192R variant)…
- Have a practitioner guide you through a pesticide or liver detox.
- Take the detox steps described above.
- Stop getting your produce from the grocery store (the people are nicer at farmer’s markets, and the farmers there give a damn about the quality of their products).
VDR
This gene governs your Vitamin D receptors, and as I’m sure you know, Vitamin D is a big deal in the baby-making business. Your personal genotyping will red flag any variants you may have that deleteriously affect your Vitamin D uptake.
You’ll need to supplement some more (especially if you don’t live someplace where you need to worry about coconuts falling on your head!) Get your Vitamin D3 levels tested; if you’re deficient (below about 70 ng/ml), supplement 5000 IU per day until you get into a healthier range.
With the major infertility-related genes addressed, let’s turn to…
Male factor infertility


The man’s genes are not an insignificant factor in fertility. So gents, if you haven’t already, book that appointment to go take a squirt in a cup in a private room at the hospital or fertility clinic to get the state of your swimmers analyzed! An interesting factoid, according to the paper, The Genetics of Infertility: Current Status of the Field
there are more than 2,300 genes expressed in the testis alone, and hundreds of those genes influence reproductive function in humans and could contribute to male infertility.
So it’s important that both partners get their genotyping done; his genome analysis will red flag the genes that might be making him not-so-dangerous in the baby-making department. Also, getting genotyping for both partners gives you the opportunity to identify which heritable conditions your future children may be at risk for – a complicated topic that is outside the scope of this article.
What conditions and genes impact male fertility…
Of the single gene disorders affecting men, the most common is classic cystic fibrosis (which affects pulmonary and lung functioning). It’s associated with the gene CFTR (your genotyping will red-flag problematic variants if you have them). If you’re diagnosed with cystic fibrosis, you’ll really need to step up your Biohacking to support your testosterone and sperm production (the tips below are a good place to start). And you may need to have a hard conversation with your urologist about this, a certain proportion of men with cystic fibrosis are sterile and will need to turn to assisted reproductive technology according to the Cystic Fibrosis Foundation.
Men can also be MTHFRers, if he carries the problematic C677-T variant he’s probably not methylating properly which may decrease his sperm count and motility. Take the steps described above to support methylation and do your damnedest to avoid consuming synthetic folic acid.
Klinefelter’s syndrome, which is relatively uncommon, affecting about one in 500 men, results in males having an extra X chromosome and causes an absence of sperm in semen. If your sperm count is in the basement, you may want to look at the gene it’s associated with, 47XXY. If you’re the rare gent stricken with this one, look into testosterone replacement therapy.
What else can men do in the fertility optimization department…
- Take testosterone-enhancing herbs: Horny Goat Weed, Tongkat Ali, and Tribulus Terrestris – they’ll make you feel like more of a man and mitigate cases of whiskey dick. Just make sure you’re getting them COA-verified as pure (the cheap stuff on Amazon very well may contain heavy metals that do you more harm than good!)
- Zinc is a big deal for men; not getting enough will impact testosterone and fertility, along with making them bitchy (less able to handle stress). Get your Zinc levels tested; if you’re below 14 mg/100 mL, supplement Zinc picolinate (a more bioavailable form of Zinc) or increase dietary Zinc – it’s generally associated with a higher-protein diet, so splurge more on the fanciest organic grass-fed beef you can afford!
- Dump the boxer briefs and let your junk dangle – boxer briefs (or whitey-tighties) hold your balls up against your body where it’s too hot for them – impacting sperm production.
- STOP drinking beer. Contrary to what the advertising might have you believe, beer is the most estrogenic booze – not good for your fertility, testosterone, and overall manly health. Switch to bio-dynamic, organic wine or vodka.
- Save your seed! Gents, semen is biologically costly for your body to produce, and if you’re struggling with fertility, your lady should be the only one that gets yours! So, it’s a great time to dump the adolescent habit of sneaking off to rub one out.
- Stress management is not just for her. As men, we are more given to a stoic mindset that just soldiers on through stress, but this may be sabotaging your fertility. We’ll turn to this topic next…
Stress management


Stress is the enemy of fertility. There’s a resounding consensus among fertility doctors, practitioners, and the scientific literature – stress is a contributing factor in almost every infertility condition. So you really need to stack multiple stress management measures…
- Quit your stressful job or cool it with the workaholism in your career.
- Habituate a mindfulness meditation practice that works for you. Dual N-Back brain training has a similar effect on stress if you really struggle to meditate.
- Breathwork practice is a game-changer for stress management; Guided breathwork sessions lasting just 5-20 minutes will stimulate you in the mornings and cool you down in the evenings or moments of overwhelm.
- Get out of toxic relationships, or at least put them on pause at least until after you’re a parent.
- Read some books about anger management (I needed this!) and anxiety. They’ll shift your mindset around the stressful emotions that you long took for granted, which “put a very high cost on very small things.”
- Uninstall YouTube, cancel your Netflix subscription and meditate or read books in the evenings instead of binging on addictive content that stimulates you before bedtime.
- Take adaptogenic herbs daily; they taste nice and will make your autonomic nervous system more resilient in this crazy world.
- 10-20 minutes of red light therapy a day has a powerful full-spectrum anti-stress effect.
- Follow the ancient wisdom about sabbatical breaks in the week. Take a day or two a week off work – go for a hike or spend some time in nature.
- Have more sex (not just when you’re trying to get pregnant) and be intentional about having better sex (men should look into Tantric practice – it’s a mindblowing hedonism health hack for greater intimacy).
- Address any underlying sources of lingering conflict with your partner. This may take having some uncomfortable conversations, listening, compromise, negotiation, or couples therapy.
- Faith and spirituality are calming sources of strength for billions of people, so get more consistent about prayer practice, devotional time, or church attendance. If you’re not religious, try the epigenetic mindset meditation developed by Dr. Joe Dispenza.
- Exercise a few times a week, but your goal in life right now is to make a baby, not complete an Iron Man race, so go a little easier.
- Be mindful of your Heart Rate Variability; this biomarker represents how well your heart and nervous system are responding to stressors, both internal and external. You can quantify and Biohack your stress with an HRV device. There’s a bunch out there that will all help, but I think the best option is probably a stylish Garmin HRV Smartwatch – which gives you a real-time “Body Budget” estimating how much stress or exercise you can handle on a given day.
Folic Acid – The New Smoking?


That’s what Dr. Carolyn Ledowsky asseverates about the epidemic of unmetabolized folic acid in the population, driving widespread systemic dysfunction of the methylation cycle. The synthetic folic acid that we get from “fortified foods” (thanks to the health “geniuses” in government food regulating agencies) and shoddy multivitamin supplements sold in white plastic bottles prevent our bodies from methylating properly. You may not carry problematic MTHFR genes, but if you’re struggling with infertility, your methylation probably has something to do with that. Fertility doctors report multitudinous cases of women who dealt with infertility for years but finally got pregnant and gave birth when they made an effort to remove folic acid from their diets.
Niacin/Vitamin B3
The epigenetic vitamin came up a lot in the expert’s recommendations for addressing fertility challenges. Supplementing it is a pretty good idea for almost everybody; if you have a smartphone and Wifi, those EMFs are causing breaks in your sperm or egg’s DNA daily, and Niacin fuels your body’s DNA repair system, PARP. You’ll get a bigger biological bang for your supplementation buck by taking the non-flush stuff (you’ll get used to the flush), NR, or NMN.


Acupuncture – a placebo that might deliver you a little bundle of joy?


I came across an interesting 2022 meta-analysis on Acupuncture as an infertility treatment, which crunched the statistically significant data of 27 randomized controlled trials totaling over 7000 human subjects. Good news: it found Acupuncture to be broadly helpful in treating infertility and improving live birth rates. However, in the meta-analysis, true Acupuncture did not outperform sham Acupuncture by much…
We found clear advantages of acupuncture over blank control conditions in terms of the live birth rate , biochemical pregnancy rate, ongoing pregnancy rate, and clinical pregnancy rate. However, these effects were similar between the true and sham acupuncture groups, and the rate of adverse events was lower in the sham group than in the true acupuncture group.
So it’s yet another case of the pragmatic Biohacker’s best friend, the placebo effect, working its magic! Thousands of women went into Acupuncture offices, got pricked with some needles, believed it was helping their fertility, and had more live births than the blank controls. So, I’m convinced that Acupuncture is worth adding to the motivated couple’s fertility optimization stack.
Further reading
Researching this topic, I turned to Enhancing Fertility through Functional Medicine by Jaclyn M. Downs and the dreadfully boring book, Fertility Genes: The Genetic Advantage (you’ll need some strong coffee to get through it!) Both clarified some things about genetics and fertility, and you may want to pick them up.
My research on fertility optimization is incomplete
At the time of publication of this article, I’m still waiting on my own whole genome sequencing due to a mix-up with the international shipping of my kit. In its current form, this article is based on cross-referencing my wife’s whole genome sequencing with my rigorous research on the topic of fertility-related genes. So expect an update and follow-up when I get mine done. Join our newsletter and subscribe to the Limitless Mindset channel, podcast, or Substack to get that follow-up (and to stay on the cutting edge with the latest in Biohacking, longevity, and lifehacking).
Conclusion


Cross-referencing your genome by common infertility-causing conditions and genes may very well reveal the needle in the haystack you need to find to put “unexplained infertility” behind you. However, genetics is complicated, and employing the counsel of a genetic counselor is wise for this journey.
If you’ve been a long-time reader of mine, I hope you pick up the through line in my writing and research. From social dynamics hacks, picking up chicks, salsa dancing, and the weird and wacky relationship hacks I write about that have kept my marriage a happy one for nearly seven years now. To epigenetic optimization for taking back your destiny, precision Biohacking with personal genotyping, and my optimistic accelerationist vision for the future of mankind on this planet. It’s all about making better little humans whose brilliance, one day, will scarcely be outshone by the cosmos. To the stars!






{kind=link}